It was Doug Hess, in Bowling Green, Ohio, who performed the first open sleeve gastrectomy in the March of 1988 as part of what is now known as the duodenal switch procedure. In 1999, the first laparoscopic approach to the duodenal switch was developed on a porcine model by de Csepel, Jossart, and Gagner. Later on, due to high complication rate of duodenal switch surgery in very obese individuals, they subsequently developed the technique of staging the intestinal bypass procedure by performing the laparoscopic sleeve gastrectomy, only as an initial stage. It was noted that LSG worked very well as a stand-alone procedure, and majority of these patients did not require the bypass procedure later.
LSG is technically easier when compared with gastric bypass or biliopancreatic diversion. It is free from serious anatomical intestinal complications in the long run like internal herniation or small bowel obstruction, and the micronutrient deficiencies and malnutrition are less frequent.
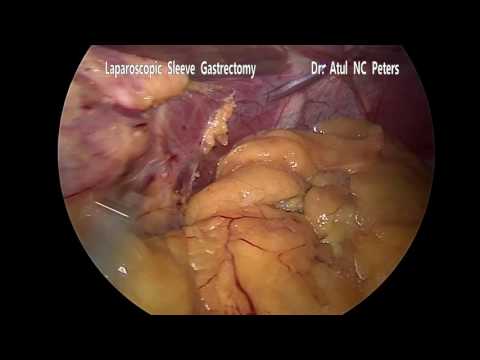
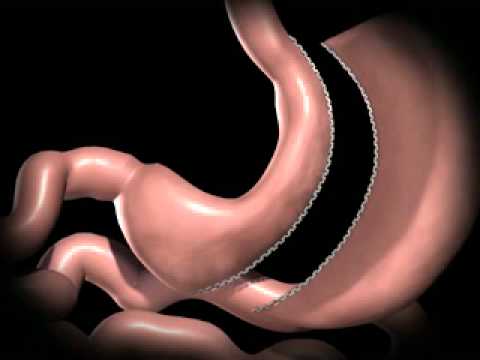
Laparoscopic/Robotic sleeve gastrectomy which is also known as vertical sleeve gastrectomy is a procedure in which about 70 to 80% of the stomach is removed leaving a narrow gastric tube or "sleeve" through which food passes. It has now become popular at most of the centres as Laparoscopic Sleeve Gastrectomy is technically easier when compared with gastric bypass or biliopancreatic diversion. It is free from serious anatomical intestinal complications in the long run like internal herniation or small bowel obstruction, and the micronutrient deficiencies and malnutrition are less frequent.
Patient position remains same as in Roux-en-Y gastric bypass. Number of incisions are 3 to 4.
The sleeve constructed with use of about 6 to 7 surgical staplers over a special tube called a gastric calibration tube. A leak test may be performed intra operatively to see that the staple line is intact in select group of patients.
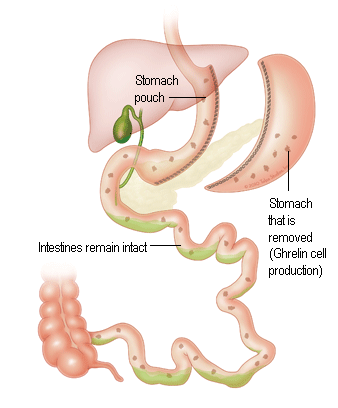
Due to this small stomach tube, the amount of food ingested is restricted and a person can take small amount of food at a time, thereby, the amount of calories consumed is restricted which results in weight loss.
The removed part of the stomach includes fundus, which is the upper outer part of stomach. It is important as it releases hormone Ghrelin. This hormone is termed as‘hunger hormone’ because it stimulates appetite, increases food intake and promotes fat storage. By removal of fundus, the source of Ghrelin is removed. No intestines are removed or bypassed during Sleeve Gastrectomy so that malabsorption is minimal.
Having said that, it is not only the restriction that causes the weight loss but many a metabolic changes also occur due to rapid transit of the food in the intestines, releasing intestinal hormones that cause these effect. Thus Sleeve Gastrectomy is no longer considered purely a restrictive surgery but also a metabolic surgery.
Though, Sleeve Gastrectomy was originally used as a first step procedure for a more definitive gastric bypass in super obese, now it is also used as a single stage procedure with excellent results across the globe. In patients with Reflux Disease and Diabetes, the results may be inferior to the Roux-en-Y Gastric Bypass but the excess weight loss of both the procedures may be comparable in a select subgroup of patients which is about 80% of the excess weight.
It is a simple procedure and the patients may be able to leave the hospital in one day or even the same day in selected cases.