Excess Body Fat Can Take Years Off Your Life
Explore the impact of excessive body fat on health, BMI classifications, and how bariatric surgery can offer long-term weight loss solutions.
Read more
Management of Diabetes After Bariatric Surgery
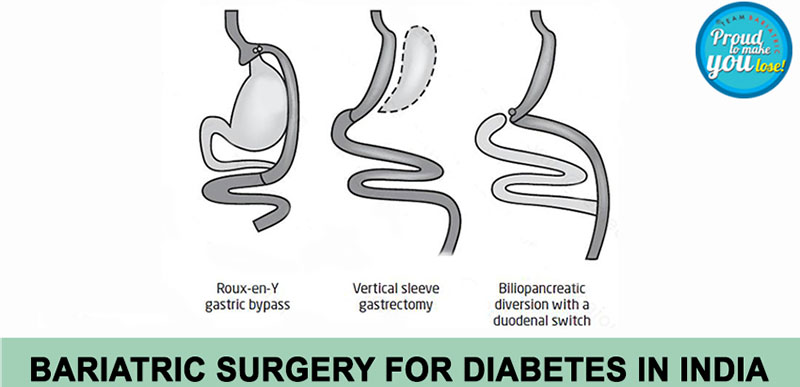
Discover essential tips for management of diabetes after bariatric surgery, including insulin adjustments and dietary guidelines.
Read more